
Urine cytology is a non-invasive diagnostic technique widely used in the detection and monitoring of urothelial carcinomas, particularly bladder cancer. By analyzing exfoliated cells from the urinary tract, this cytopathological method provides valuable insights into malignant and premalignant processes. Despite the emergence of advanced molecular diagnostics, urine cytology remains an essential tool due to its high specificity for high-grade urothelial carcinoma and its role in routine clinical practice.
This article reviews the principles, diagnostic applications, and limitations of urine cytology in the context of urinary tract neoplasms.
I. Principles of Urine Cytology
1.1 Cytopathological Basis
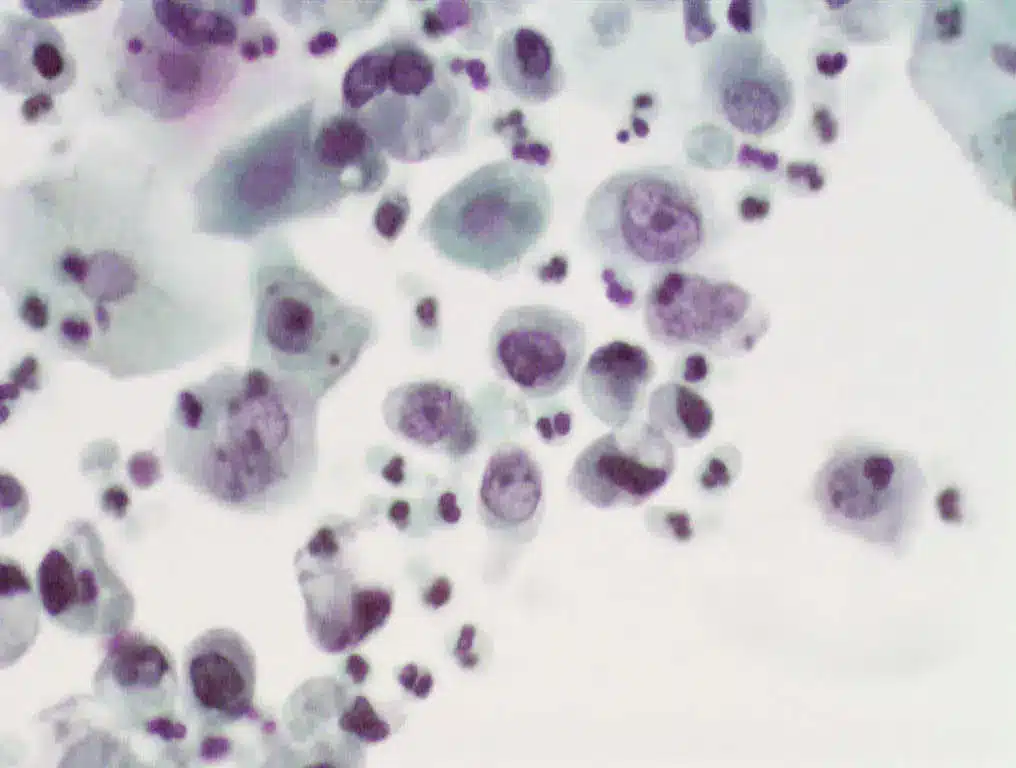
Urine cytology is grounded in the principles of cytopathology, where individual exfoliated cells from the urinary tract are examined microscopically. The urinary tract epithelium, primarily composed of urothelial cells, continuously sheds cells into the urine, providing a diagnostic sample. The assessment focuses on cellular morphology, identifying features such as nuclear enlargement, hyperchromasia, and irregular nuclear contours that are indicative of malignancy.
Staining methods, particularly the Papanicolaou stain, enhance the visualization of cellular detail and allow for the distinction between benign, reactive, and malignant cells. Hematoxylin and eosin staining may be used adjunctively in some laboratories.
1.2 Sample Collection and Preparation
The quality of a urine cytology specimen significantly influences diagnostic accuracy. Samples can be obtained from voided urine, catheterized urine, or bladder washing, with bladder washing providing the highest cellular yield but being more invasive.
Proper sample handling includes immediate fixation to preserve cellular morphology and prevent degradation. Liquid-based cytology techniques, such as ThinPrep® or SurePath®, have improved specimen preparation, reducing artifacts and improving cellular representation compared to conventional smears.
Variables such as specimen turbidity, contamination by inflammatory cells, or degenerated cells from infection can compromise sample adequacy and complicate interpretation.
II. Diagnostic Interpretation of Urine Cytology
2.1 Normal Urinary Cytology
Normal urine cytology specimens contain urothelial cells, squamous epithelial cells, and occasional inflammatory cells. Normal urothelial cells are small to medium-sized with uniform nuclei, smooth nuclear contours, and a moderate amount of cytoplasm. Recognizing these baseline features is essential for distinguishing pathological alterations.

2.2 Cytological Abnormalities
Urine cytology primarily targets the detection of urothelial carcinoma, with a focus on high-grade urothelial carcinoma (HGUC). Malignant cells exhibit increased nuclear-to-cytoplasmic ratios, hyperchromatic nuclei, coarse chromatin, and irregular nuclear membranes.
- Atypical urothelial cells may display subtle nuclear changes but fall short of diagnostic criteria for carcinoma. These findings often warrant further investigation.
- Low-grade urothelial carcinomas, however, shed few cells with mild atypia, making them difficult to detect cytologically.
- Cytology can also reveal malignant cells from tumors of the renal pelvis, ureters, or urethra, although these are less common.
2.3 Reporting Systems
The Paris System for Reporting Urinary Cytology (TPS) has standardized diagnostic categories to improve clarity and clinical correlation. Categories include:
- Negative for High-Grade Urothelial Carcinoma
- Atypical Urothelial Cells
- Suspicious for High-Grade Urothelial Carcinoma
- High-Grade Urothelial Carcinoma
- Low-Grade Urothelial Neoplasia (rarely diagnosed by cytology)
- Other malignancies (e.g., squamous cell carcinoma, adenocarcinoma)
TPS emphasizes sensitivity for high-grade malignancies, reflecting the clinical utility of urine cytology in detecting aggressive tumors.
III. Clinical Applications and Diagnostic Accuracy
3.1 Role in Bladder Cancer Diagnosis
Urine cytology plays a pivotal role in the diagnosis and surveillance of bladder cancer, particularly high-grade urothelial carcinoma (HGUC). Its high specificity makes it an important tool for confirming malignancy in patients presenting with hematuria or as part of routine follow-up for patients with a history of non-muscle invasive bladder cancer (NMIBC). However, the sensitivity of urine cytology for detecting low-grade urothelial tumors remains limited, as these tumors shed fewer atypical cells into the urine.
3.2 Differential Diagnosis
Urine cytology also aids in differentiating malignant lesions from benign conditions such as urinary tract infections (UTIs), nephrolithiasis, or reactive changes due to instrumentation. Reactive atypia, inflammation, and cellular degeneration can mimic malignancy, underscoring the importance of integrating cytology findings with clinical and cystoscopic data.
3.3 Comparison with Other Diagnostic Modalities
While cystoscopy remains the gold standard for bladder cancer diagnosis, urine cytology offers a non-invasive adjunctive tool, especially valuable when cystoscopy findings are inconclusive or when patients require long-term surveillance.
Newer diagnostic markers, such as NMP22, telomerase activity assays, and FGFR3 mutation analysis, have been introduced to complement urine cytology, improving the sensitivity for detecting bladder cancer. However, cytology remains particularly reliable for identifying high-grade tumors, where its performance surpasses that of many molecular markers.
IV. Advantages and Limitations of Urine Cytology
4.1 Advantages
Urine cytology is a non-invasive, low-risk, and cost-effective diagnostic tool, making it well-suited for routine clinical use. Its main strength lies in its high specificity, particularly for high-grade urothelial carcinoma (HGUC), where the presence of markedly atypical cells allows for a confident diagnosis. Additionally, urine cytology can detect malignancies originating from various parts of the urinary tract, including the renal pelvis, ureters, and bladder, providing a broad diagnostic window.
It also serves as a useful surveillance tool in patients with a history of bladder cancer, aiding in the early detection of tumor recurrence during follow-up.
4.2 Limitations
Despite its advantages, urine cytology has significant limitations, most notably its low sensitivity for low-grade urothelial tumors, which often fail to exfoliate diagnostically abnormal cells. As a result, early or well-differentiated cancers may go undetected.
Other limitations include:
- Subjectivity in interpretation, requiring experienced cytopathologists for accurate diagnosis.
- The potential for false positives, particularly in cases of severe inflammation, prior instrumentation, or urinary tract infections, where reactive changes may mimic malignancy.
- The possibility of false negatives, particularly in cases with inadequate specimens or low tumor cell shedding.
These limitations highlight the importance of using urine cytology in conjunction with other diagnostic modalities such as cystoscopy, biopsy, and molecular assays to improve diagnostic accuracy.
V. Recent Advances and Future Perspectives
5.1 Advances in Cytology Techniques
Technical improvements in urine cytology have enhanced specimen quality and diagnostic accuracy. Liquid-based cytology (LBC) methods, such as ThinPrep® and SurePath®, reduce background debris and allow for better cell preservation and distribution on slides. These methods improve detection rates, particularly in challenging cases.
Adjunctive techniques like immunocytochemistry (e.g., staining for p53, cytokeratin, or Ki-67) help differentiate malignant from reactive urothelial cells. Additionally, digital cytology and machine learning algorithms are being explored to assist pathologists in identifying atypical cells, potentially reducing interobserver variability.
5.2 Emerging Urinary Biomarkers
Several urinary biomarkers have been developed to complement cytology and increase sensitivity, especially for low-grade tumors. Among them:
- FGFR3 mutations, frequently found in low-grade bladder cancers.
- NMP22 (Nuclear Matrix Protein 22), associated with urothelial tumor cell turnover.
- Telomerase activity, indicative of cellular immortality in malignancies.
- Emerging approaches such as circulating tumor DNA (ctDNA), exosomal RNA, and microRNA profiling, which offer promising non-invasive options.
Integration of next-generation sequencing (NGS) and multi-omics approaches with cytology could lead to more comprehensive and personalized diagnostic strategies for urinary tract malignancies.
Conclusion
Urine cytology remains a cornerstone in the non-invasive diagnosis and surveillance of urothelial carcinomas, offering high specificity for high-grade malignancies. While its sensitivity for low-grade tumors is limited, ongoing advancements in cytological techniques and the integration of molecular biomarkers continue to enhance its diagnostic value. Future developments combining cytopathology with molecular diagnostics hold promise for more precise and comprehensive urinary tract cancer detection.
References
- Planz B, Jochims E, Deix T, Caspers HP, Jakse G, Boecking A. The role of urinary cytology for detection of bladder cancer. Eur J Surg Oncol. 2005 Apr;31(3):304-8. doi: 10.1016/j.ejso.2004.12.008. PMID: 15780568.
- Barkan GA, Wojcik EM, Nayar R, Savic-Prince S, Quek ML, Kurtycz DF, Rosenthal DL. The Paris System for Reporting Urinary Cytology: The Quest to Develop a Standardized Terminology. Acta Cytol. 2016;60(3):185-97. doi: 10.1159/000446270. Epub 2016 Jun 18. PMID: 27318895.
- Koss, L. G. (2006). Diagnostic Cytology and Its Histopathologic Bases (5th ed.). Lippincott Williams & Wilkins.
- Lotan, Y., & Roehrborn, C. G. (2003). Sensitivity and specificity of commonly available bladder tumor markers versus cytology: Results of a comprehensive literature review and meta-analyses. Urology, 61(1), 109–118. https://doi.org/10.1016/s0090-4295(02)02136-2
- Xylinas E, Kluth LA, Rieken M, Karakiewicz PI, Lotan Y, Shariat SF. Urine markers for detection and surveillance of bladder cancer. Urol Oncol. 2014 Apr;32(3):222-9. doi: 10.1016/j.urolonc.2013.06.001. Epub 2013 Sep 17. PMID: 24054865.
- Barkan, G. A., et al. (2016). The Paris System for Reporting Urinary Cytology: The Quest to Develop a Standardized Terminology. Cytopathology, 27(1), 1–13. https://doi.org/10.1111/cyt.12445
- Burger, M., et al. (2013). Epidemiology and risk factors of urothelial bladder cancer. European Urology, 63(2), 234–241. https://doi.org/10.1016/j.eururo.2012.07.033

{kind=link}