

In recent years, CAR-T cell therapy—short for Chimeric Antigen Receptor T-cell therapy—has emerged as one of the most promising innovations in cancer immunotherapy. Unlike conventional treatments such as chemotherapy or radiotherapy, CAR-T therapy harnesses the patient’s own immune system by genetically reprogramming T lymphocytes to specifically recognize and eliminate malignant cells.
Since its first FDA approval in 2017, CAR-T therapy has shown remarkable clinical success, particularly in hematologic malignancies such as B-cell acute lymphoblastic leukemia (B-ALL), diffuse large B-cell lymphoma (DLBCL), and multiple myeloma. Several therapies—including Kymriah, Yescarta, Tecartus, Breyanzi, Abecma, and Carvykti—are now available, representing a new era of personalized medicine.
Despite these advances, CAR-T therapy faces challenges, including severe toxicities such as cytokine release syndrome (CRS) and neurotoxicity, high manufacturing costs, and limited efficacy against solid tumors. Ongoing research aims to overcome these barriers by developing next-generation CAR-T cells, incorporating gene-editing tools like CRISPR, and exploring combination therapies.
This article provides an in-depth look at the mechanism of CAR-T therapy, clinical applications, adverse effects, and future directions, offering valuable insights for students, clinicians, and researchers in the biomedical sciences.
What is CAR-T Cell Therapy?
CAR-T cell therapy (Chimeric Antigen Receptor T-cell therapy) is a type of adoptive cell transfer immunotherapy in which a patient’s own T lymphocytes are collected, genetically modified, and reinfused to target cancer cells. The central innovation lies in the introduction of a synthetic receptor, called a Chimeric Antigen Receptor (CAR), that enables T cells to recognize tumor-associated antigens independently of the major histocompatibility complex (MHC).
The therapeutic process involves several steps:
- Leukapheresis – harvesting the patient’s T cells.
- Genetic modification – insertion of CAR genes (commonly using lentiviral or retroviral vectors) to reprogram T cells.
- Ex vivo expansion – growing millions of modified CAR-T cells in controlled laboratory conditions.
- Infusion – reinfusing the engineered cells back into the patient after a preparatory chemotherapy regimen.

CARs are designed with multiple functional domains:
- Extracellular antigen-binding domain (usually derived from a monoclonal antibody’s single-chain variable fragment, scFv).
- Transmembrane domain anchoring the receptor.
- Intracellular signaling domains (such as CD3ζ, CD28, or 4-1BB) that trigger T-cell activation and proliferation upon antigen recognition.
CAR-T Therapy vs. Other Immunotherapies
Unlike immune checkpoint inhibitors, which release natural brakes on T-cell activity, CAR-T therapy actively engineers immune cells for tumor-specific targeting. This provides higher specificity but also carries risks of unique toxicities, making it distinct within the landscape of modern cancer immunotherapies.
Mechanism of Action of CAR-T Cell Therapy
The therapeutic power of CAR-T cells lies in their ability to precisely recognize and destroy malignant cells. Unlike natural T-cell receptors, which depend on antigen presentation via the MHC complex, the engineered Chimeric Antigen Receptor (CAR) enables T cells to directly bind to specific tumor-associated antigens expressed on cancer cells.
Step-by-Step Mechanism
- Antigen Recognition
- CARs are designed to target surface proteins such as CD19 (expressed on B-cell malignancies), CD20, or BCMA (B-cell maturation antigen, relevant in multiple myeloma).
- Once infused into the patient, CAR-T cells patrol the bloodstream and bind directly to these tumor antigens via their extracellular scFv domain.
- T-Cell Activation and Signal Transduction
- Antigen binding triggers the intracellular signaling domains of the CAR (e.g., CD3ζ).
- Co-stimulatory molecules such as CD28 or 4-1BB further enhance T-cell proliferation, persistence, and survival.
- Cytotoxic Response
- Activated CAR-T cells release perforins and granzymes, leading to direct lysis of cancer cells.
- They also secrete a cascade of cytokines such as IL-2, IFN-γ, TNF-α, and IL-6, amplifying the immune response.
- Clonal Expansion and Persistence
- The CAR-T cells proliferate in vivo, creating a durable population of tumor-specific T cells.
- This persistence is crucial for preventing relapse and maintaining long-term remission.
The Role of Cytokines
While cytokine release is essential for tumor clearance, it can also lead to severe toxicities. The excessive production of IL-6 and other inflammatory mediators underlies Cytokine Release Syndrome (CRS), a major clinical challenge in CAR-T therapy.
Key Targets and Examples
- CD19-directed CAR-T: successful in treating B-ALL and DLBCL.
- BCMA-directed CAR-T: effective against multiple myeloma.
- Ongoing trials are exploring novel targets for solid tumors, though the tumor microenvironment remains a significant barrier.
Clinical Applications of CAR-T Therapy
Since its first approval, CAR-T cell therapy has transformed the management of several hematologic malignancies. The ability to redirect T cells against specific tumor antigens has led to unprecedented remission rates in patients with relapsed or refractory cancers. However, extending these benefits to solid tumors remains a major challenge.
CAR-T in Hematologic Malignancies
- B-cell Acute Lymphoblastic Leukemia (B-ALL)
- CD19-directed CAR-T therapy has shown remarkable efficacy in pediatric and young adult patients with relapsed or refractory B-ALL.
- Clinical trials demonstrated complete remission rates exceeding 80%, leading to the approval of tisagenlecleucel (Kymriah).
- Diffuse Large B-cell Lymphoma (DLBCL)
- Patients with relapsed/refractory DLBCL, traditionally difficult to treat, have benefited from therapies such as axicabtagene ciloleucel (Yescarta) and lisocabtagene maraleucel (Breyanzi).
- Durable responses have been observed, with significant improvements in progression-free survival.
- Multiple Myeloma
- Targeting BCMA (B-cell maturation antigen) has emerged as a breakthrough for patients with relapsed or refractory multiple myeloma.
- Idecabtagene vicleucel (Abecma) and ciltacabtagene autoleucel (Carvykti) represent the first FDA-approved BCMA-directed CAR-T therapies.
Challenges in Solid Tumors
While CAR-T therapy has revolutionized the treatment blood cancers, its application in solid tumors has been limited due to several obstacles:
- Tumor Microenvironment (TME): Physical barriers, immunosuppressive cytokines, and regulatory T cells hinder CAR-T infiltration and activity.
- Antigen Heterogeneity: Unlike CD19 or BCMA, many solid tumors lack a uniform and specific antigen target.
- On-target, Off-tumor Toxicity: Potential recognition of antigens expressed on normal tissues increases the risk of collateral damage.
Ongoing clinical trials are exploring innovative strategies such as armored CAR-T cells, dual-targeted CARs, and combination immunotherapies to overcome these hurdles.
FDA-Approved CAR-T Cell Therapies
The approval of CAR-T therapies by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) has marked a turning point in oncology. These therapies are no longer experimental but are now part of standard care for selected hematologic malignancies. Below is an overview of currently approved CAR-T products, their targets, and clinical indications.
1. Tisagenlecleucel (Kymriah, Novartis)
- Target antigen: CD19
- Approved for:
- Pediatric and young adult patients with relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL)
- Adults with relapsed/refractory diffuse large B-cell lymphoma (DLBCL)
- Key point: First CAR-T therapy to receive FDA approval (2017).
2. Axicabtagene Ciloleucel (Yescarta, Kite/Gilead)
- Target antigen: CD19
- Approved for: Adults with relapsed/refractory DLBCL and certain subtypes of large B-cell lymphoma
- Key point: Demonstrated high overall response rates in patients refractory to multiple prior lines of therapy.
3. Brexucabtagene Autoleucel (Tecartus, Kite/Gilead)
- Target antigen: CD19
- Approved for:
- Mantle cell lymphoma (MCL)
- B-cell precursor ALL in adults (later approval)
- Key point: First CAR-T therapy approved specifically for mantle cell lymphoma.
4. Lisocabtagene Maraleucel (Breyanzi, Bristol Myers Squibb)
- Target antigen: CD19
- Approved for: Relapsed/refractory large B-cell lymphoma after ≥2 prior lines of therapy
- Key point: Notable for controlled dosing of CAR-T cell subsets (CD4+ and CD8+) to optimize safety and efficacy.
5. Idecabtagene Vicleucel (Abecma, Bristol Myers Squibb/Bluebird Bio)
- Target antigen: BCMA (B-cell maturation antigen)
- Approved for: Relapsed/refractory multiple myeloma after at least four prior therapies
- Key point: First FDA-approved BCMA-directed CAR-T therapy.
6. Ciltacabtagene Autoleucel (Carvykti, Janssen/Legend Biotech)
- Target antigen: BCMA
- Approved for: Patients with multiple myeloma after multiple prior lines of therapy
- Key point: Distinctive dual-epitope targeting for enhanced antigen binding and potency.
Global Perspective and Regulatory Landscape
- Both the FDA and EMA have expanded approvals to cover multiple indications within hematologic cancers.
- Pharmaceutical leaders in the CAR-T field include Novartis, Gilead/Kite, Bristol Myers Squibb, and Janssen.
- Ongoing trials are likely to expand approvals to earlier lines of treatment and possibly into solid tumors.
Adverse Effects and Safety Considerations
Sec. Cancer Immunity and Immunotherapy
Volume 13 – 2022 | https://doi.org/10.3389/fimmu.2022.1079181
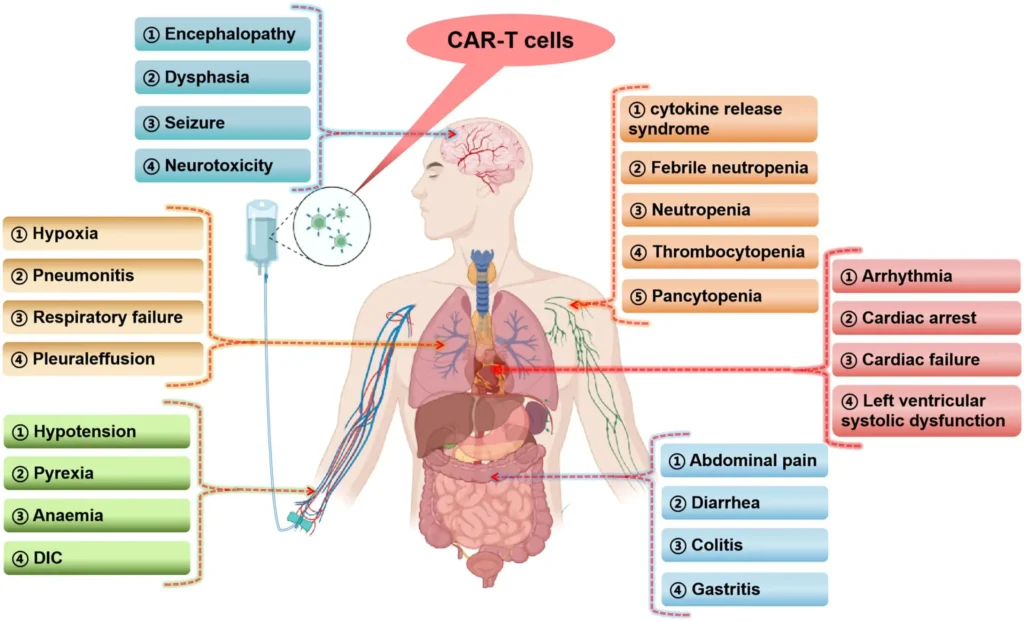
While CAR-T cell therapy has achieved remarkable success in treating hematologic cancers, its clinical use is often complicated by unique and potentially life-threatening toxicities.
1. Cytokine Release Syndrome (CRS)
- Definition: A systemic inflammatory response caused by massive cytokine secretion following CAR-T activation and tumor lysis.
- Pathophysiology: Elevated levels of IL-6, IL-1, IFN-γ, and TNF-α drive fever, hypotension, hypoxia, and multi-organ dysfunction.
- Clinical presentation: High fever, tachycardia, hypotension, capillary leak, and organ failure in severe cases.
- Management:
- Tocilizumab (anti–IL-6 receptor antibody) is the mainstay of treatment.
- Corticosteroids are used in refractory cases.
- Supportive care in intensive care units for severe CRS.
2. Neurotoxicity (Immune Effector Cell-Associated Neurotoxicity Syndrome, ICANS)
- Definition: A spectrum of neurological complications seen after CAR-T infusion.
- Symptoms: Confusion, aphasia, seizures, cerebral edema in severe cases.
- Mechanism: Thought to involve cytokine-mediated blood–brain barrier disruption.
- Management:
- Corticosteroids (e.g., dexamethasone) are the primary intervention.
- Tocilizumab is less effective for neurotoxicity, as IL-6 blockade does not fully penetrate the central nervous system.
3. On-target, Off-tumor Toxicity
- CAR-T cells may attack normal tissues expressing low levels of the targeted antigen.
- This is particularly concerning in solid tumors, where antigens are rarely tumor-specific.
4. Long-Term Risks
- Prolonged cytopenias due to marrow suppression.
- Hypogammaglobulinemia from B-cell aplasia in CD19-directed CAR-T therapy, requiring IV immunoglobulin replacement.
- Potential secondary malignancies, though evidence remains limited.
Safety Strategies in CAR-T Development
- Incorporation of suicide genes or safety switches (e.g., inducible caspase-9 systems).
- Optimized dosing regimens and careful patient selection.
- Next-generation CAR-T designs that enhance tumor specificity while minimizing collateral damage.
Limitations and Challenges of CAR-T Therapy

Sec. Hematologic Malignancies
Volume 14 – 2024 | https://doi.org/10.3389/fonc.2024.1397613
Despite its transformative impact on hematologic oncology, CAR-T cell therapy faces several biological, clinical, and practical limitations that hinder its widespread application. These challenges highlight the need for continued research and innovation.
1. Cost and Accessibility
- High cost of CAR-T therapy remains a major barrier, with single treatments often exceeding $350,000–$500,000 USD, excluding hospitalization and supportive care.
- Complex manufacturing processes (patient-specific T-cell engineering, ex vivo expansion) limit scalability.
- Disparities in access persist globally, especially in low- and middle-income countries.
2. Relapse and Resistance
- Some patients relapse due to antigen escape, where tumor cells lose or downregulate the targeted antigen (e.g., CD19-negative relapses after CD19-directed CAR-T).
- T-cell exhaustion and limited persistence reduce long-term efficacy.
- The tumor microenvironment (TME), particularly in solid tumors, provides immunosuppressive barriers that limit CAR-T activity.
3. Toxicities and Clinical Risk
- Cytokine Release Syndrome (CRS) and Neurotoxicity (ICANS) remain significant risks despite improvements in supportive management.
- On-target, off-tumor toxicity poses challenges in identifying truly tumor-specific antigens.
4. Ethical and Logistical Issues
- Questions regarding fair distribution, cost-effectiveness, and long-term patient monitoring raise ethical concerns.
- Delays in manufacturing may endanger patients with rapidly progressing disease.
- Informed consent is complex, given the unpredictable risks and experimental nature of newer CAR-T platforms.
5. Limited Success in Solid Tumors
- Most clinical success has been restricted to hematologic malignancies, with limited efficacy in solid tumors due to:
- Antigen heterogeneity
- Physical barriers of the tumor microenvironment
- Risk of collateral damage to normal tissues
6. Regulatory and Production Challenges
- CAR-T therapies require stringent regulatory oversight by agencies such as the FDA and EMA.
- Manufacturing delays, batch variability, and quality control remain obstacles to broader adoption.
Conclusion
CAR-T cell therapy represents a paradigm shift in cancer treatment, offering unprecedented efficacy in hematologic malignancies and opening new avenues for personalized immunotherapy. While challenges such as cytokine release syndrome, neurotoxicity, high costs, and limited solid tumor efficacy remain, ongoing innovations—including next-generation CAR-T designs, gene editing, and combination strategies—promise to enhance safety, durability, and accessibility. As research advances, CAR-T therapy is poised to become an integral component of modern oncology, bridging the gap between cutting-edge science and clinical practice.
References
- Sterner RC, Sterner RM. CAR-T cell therapy: current limitations and potential strategies. Blood Cancer J. 2021 Apr 6;11(4):69. doi: 10.1038/s41408-021-00459-7.
- Chohan KL, Siegler EL, Kenderian SS. CAR-T Cell Therapy: the Efficacy and Toxicity Balance. Curr Hematol Malig Rep. 2023 Apr;18(2):9-18. doi: 10.1007/s11899-023-00687-7.
- Dabas P, Danda A. Revolutionizing cancer treatment: a comprehensive review of CAR-T cell therapy. Med Oncol. 2023 Aug 22;40(9):275. doi: 10.1007/s12032-023-02146-y.
- Ma S, Li X, Wang X, Cheng L, Li Z, Zhang C, Ye Z, Qian Q. Current Progress in CAR-T Cell Therapy for Solid Tumors. Int J Biol Sci. 2019 Sep 7;15(12):2548-2560. doi: 10.7150/ijbs.34213.
- https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/approved-cellular-and-gene-therapy-products

{kind=link}